BCPS 2013: Cardiology I
/A little in the past on my study schedule, but what I'm studying this past week. Acute Decompensated Heart Failure
| Parameter | Normal | ADHF | |
| MAP | 80-100 | 60-80 | |
| HR | 60-80 | 70-90 | |
| CO/CI | 4-7 / 2.8-3.6 | 2-4 / 1.3-2 | Low cardiac output |
| PCWP | 8-12 | 18-30 | Congestion |
| SVR | 800-1200 | 1500-3000 | |
| CVP | 2-6 | 6-15 | Fluid up |
*want PCWP 15-18 for optimal filling pressure
Signs and symptoms
| Congestion (PCWP) | Hypoperfusion (CO) |
| Dyspnea | Fatigue |
| Peripheral edema | Cold extremities |
| Rales | Narrow pulse pressure |
| Ascites | Hypotension |
| Jugular venous distention | Worsening renal function |
| Hepatomegaly, splenomegaly | Hyponatremia |
Subsets and Therapy
| Warm (CI > 2.2) | Cold (CI < 2.2) | |||
| Wet (PCWP > 18) | Congestion
IV diuretics + IV vasodiliators (venous) |
Congestion and Hypoperfusion | ||
| MAP < 50 | Dopamine | |||
| MAP > 50 | Inotrope* or vasodilator (V or A) | |||
| Dry (PCWP < 18) | Normal
Optimize oral meds |
Hypoperfusion | ||
| PCWP < 15 | IV fluids | |||
| PCWP > 15, MAP < 50 | Dopamine | |||
| PCWP > 15, Map > 50 | Inotrope* or vasodilator (arterial) | |||
*SBP < 90, hypotension, worsening renal function
Home HF meds in ADHF
- ACEi – caution with uptitration during diuresis and if Scr # more than 0.5 mg/dL above baseline
- BBlockers – Do not discontinue if stable prior to admission, do not start until euvolemic, hold if hemodynamically unstable
- Digoxin – goal conc 0.5-0.8 ng/mL, avoid discontinuation, caution if renal function worsens
Drugs for ADHF
Diuretics – congestion
| Loop | Furosemide 40 PO = Furosemide 20 IV = Bumetanide 1 mg = Torsemide 10 mg |
| Thiazide | Not effective if CrCl < 30, used as adjunct
HCTZ 12.5-25 mg PO, metolazone 2.5-5 mg PO Chlorothiazide 250-500 mg IV if GI edema (expensive) |
| Resistance to diuretics | Fluid and sodium restriction
Increase dose, frequency, cont infusion Add thiazide |
Inotropes – hypoperfusion
| Dobutamine
B1 agonist: inotropic, lusitropic, chronotropic |
Dose: 2.5-20 mcg/kg/min
AE: tachycardia, arrhythmia, myocardial ischemia Consider if hypotension |
| Milrinone
PDE inhibitor: inotropic, lusitropic
|
AE: arrhythmia, hypotension
Dose: 0.1-0.75 mcg/kg/min Consider if on B-blocker |
Vasodilators – congestion, (Venous $ PCWP for dyspnea), (Arterial $ SVR for $ CO)
| Nitroprusside
Arterial = venous |
Doses: 0.3-3 mcg/kg/min
AE: hypotension, cyanide/thiocyanate toxicity |
| Nesiritide
# Na excretion, UOP, CI $ PCWP, SVR, NE, aldosterone |
Doses: 0.01 mcg/kg/min
AE: hypotension, some tachycardia |
| Nitroglycerine
Venous > arterial (art w/ high doses) |
Doses: 5-200 mcg/min
AE: hypotension, reflex tachycardia, HA |
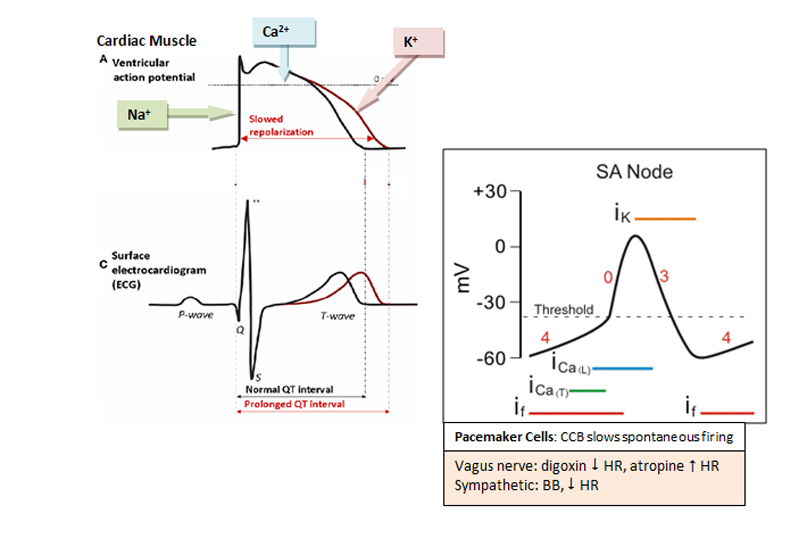
Arrhythmias
Drug therapy overview
- Check thyroid function, K 4-5 mmol/L, Mg > 2 mg/dL, QTc < 500 ms
- Potential drug causes: QTc prolongation, bradycardia, AV block
See figures on last page.
See Table 9.
Treatment of arrhythmias
| Pulseless VT/VF | Epinephrine, Vasopressin, Amiodarone, Lidocaine, eval reversible causes |
| PEA | Epinephrine, Vasopressin, eval reversible causes |
| Sx Bradyarrhythmia | If unstable: atropine 0.5-1.0 mg IV, repeat up to 3.0 mg |
| Sx Tachycardia | If unstable: cardioversion
If stable: narrow/regular (SVT) – Vagal maneuvers, adenosine, β blockers, CCB, ablation Note: avoid CCB and digoxin if WPW, adenosine 6/12 mg (caution in severe CAD) |
| Afib (narrow/irregular) |
IA (quinidine, procainamide), IC (flecainide, propofenone), III (amiodarone, sotalol, ibutalide, dofetilide)
|
| Vtach, Vfib | Cardiovert (shock) patients, give Epi or vasopressin as needed
Consider amiodarone or lidocaine during CV and after for prophy Patients with LVEF < 30 to 40% should have implantable cardioverter defibrillator (ICD) |
| Torsades | Mg |
| Special populations | HF – amiodarone and dofetilide (LV dysfxn post MI) neutral effect on mortality
Post MI – ecainide, flecainide, moricizine, 1A meds # mortality Dofetilide neutral mortality LV dysfxn post MI |
Pulmonary Arterial Hypertension
Signs and symptoms
Dyspnea w/ exertion, fatigue, chest pain, syncope, weakness, orthopnea, peripheral edema (fluid backs up), liver congestion, ascites, hemodynamics (mPAP > 25, PCWP < 15, PVR > 3), RV hypertrophy
Treatment
Goal: relieve acute dyspnea, improve exercise capacity and QOL
Vasodilator response testing: epoprostenol, inhaled nitric oxide, IV adenosine
Initial treatment algorithm
| Supportive care | |
| Oxygen | |
| Anticoagulation: warfarin goal INR 1.5-2.5 to prevent catheter thrombosis, VTE | |
| Immunizations | |
| Birth control | |
| Oral CCB | |
| If no sustained response to CCB: | |
| Low risk | High risk |
| 1st line: ERA or PDEIs (oral)
Alt: epoprostenol, treprostinil (IV) iloprost (inhaled), treprostinil (SC) |
1st line: epoprostenol, treprostinil (IV)
Alt: ERA or PDEIs (oral) iloprost (inhaled), treprostinil (SC) |
ERA: endothelin receptor antagonist (e.g. sentans) PDEIs (e.g. sildenafil)
Prostacyclin analogs (e.g. epoprostenol)
See Table 16.
Hypertensive Crises (Urgency and Emergency)
HTN urgency: acute elevation in BP > 180/120 without organ damage
HTN emergency: HTN with organ damage (encephalopathy, intracranial hemorrhage, angina or MI, pulm edema, aortic dissection, retinopathy, $ UOP or AKI, eclampsia)
Treatment
Urgency: goal to $ BP within 24 hrs
Agents (Table 18): captopril, clonidine, minoxidil, nifedipine, labetalol
Emergency: goal to $ MAP 25% or diastolic BP to 100-110 mmHg within 30-60 min
Agents (Table 17): sodium nitroprusside, esmolol, labetalol, nicardipine, nitroglycerin, hydralazine, enalaprilat, fenoldopam, clevidipine
Preferred agents for crises based on comorbidities
| Acute aortic dissection | Esmolol alone or w/ nicardipine or nitroprusside
(BB first!) |
| Acute HF | Nitroprusside, nitroglycerin, nesiritide, ACEi with diuretics if pulm edema (no BBs) |
| Stroke (ischemic, hemorrhagic) | Labetalol, nicardipine |
| Acute MI | BB with nitro, if HR < 70 nicardipine, clevidipine |
| Acute pulm edema | Nesiritide, nitroglycerin, nitroprusside |
| AKI | Fenoldopam, nicardipine, clevidipine |
| Eclampsia | Hydralazine, labetalol, nicardipine |
| HTN encephalopathy | Nitroprusside, labetalol, fenoldopam, nicardipine |
| Perioperative HTN | Clevidipine, esmolo, nicardipine, nitro |
| Sympathetic crisis | Nicardipine and such (avoid unopposed BB) |
Cardiac Muscle






 http://www.bcpsstudygroup.com/
http://www.bcpsstudygroup.com/