BCPS 2013: Infectious Diseases
/My infectious disease review. I've already talked about pneumonia and may be revising these to go from the direction of the bugs and then the drugs again. One thing I will say: Invanz is not active against MRSA, ampicillin-resistant enterococci, Pseudomonas aeruginosa or Acinetobacter species. Hear me? :)
BCPS ID Review
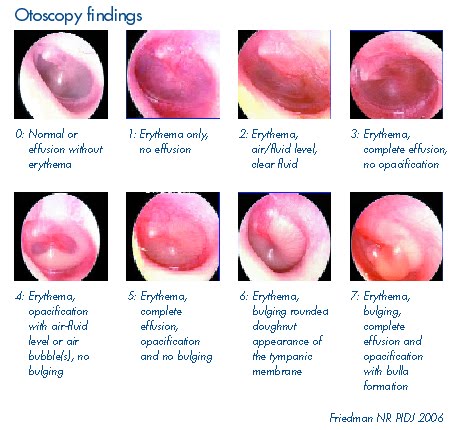
| Pneumonia |
CAP |
HAP |
| Organisms | M. pneumonia, S. pneumonia, H.flu, C. pneumonia, Legionella, Viruses | S. aureus, Pseudomonas, Enterobacter, Klebsiella pneumo, Candida, Acinetobacter, Serratia, E.coli, S.pneumonia |
| Treatment | Healthy no Abx in previous 3 months
Macrolide (clarith or azith) OR doxycycline Cormorbidity or Abx in previous 3 months FQ (moxi, gemi, levo 750mg) Macrolide (or doxy) + [High-dose amox 1g tid OR amox/clav 2g bid OR ceph ] (ceftriaxone, cefuroxime, cefpodoxime) |
Early onset (< 5 days)
3rd ceph (ceftriaxone, cefotaxime) FQ (levo, moxi, cipro) Amp/sulbactam Ertapenem Late onset (> 5 days or RF for MDR) Ceftazidime OR cefepime + AG or FQ (cipro, levo) Imi, mero, or dori + AG or FQ (cipro, levo) Pip/taz + AG or FQ (cipro, levo) + Vanco/linezolid only if MRSA risk factors |
| Duration | At least 5 days | 7 days (14 days for Pseudomonas) |
Influenza: Type A (Annual, H1N1, H1N2), Type B
Prophylaxis: if outbreak and cannot receive vaccine
1. Amantadine, Rimantadine 5-7 weeks
2. Neuraminidase inhibitors: Oseltamivir 75-150mg daily x6wks; 75mg daily x7days within 2 days of contact
Zanamivir 10mg daily through inhalation x4wks
Treatment: only if severe symptoms or at risk for complications
1. Amantadine, Rimantadine- only against Type A, decreases symptoms 1 day *do NOT use for at risk for complications
Dosing: 100mg bid x3-7 days [Elderly 100 daily]; ADJUST FOR RENAL DISEASE (amantadine> rimantadine)
AE: CNS, GI, peripheral edema, orthostatic hypotension
2. Oseltamivir- decreases symptoms 1-1.5 days
Dosing: 75mg bid x5days [CrCl <30 75mg daily]
AE: GI
3. Zanamivir- decreases symptoms 1-1.5 days
Dosing: 2 inhalations (5mg/inhalation) bid x5days
AE: bronchospasm, cough
| UTIs | Treatment | Other | Comment |
| Uncomplicated cystitis | Nitrofurantoin 100mg bid
X 5 days TMP/SMX DS bid x 3 days Or Fosfomycin 3 gm once Duration: 3 days vs 5 |
Alternatives:
Amox-clavulanate, cefdinir, cefaclor, or cefpodoxime x 3-7d or FQ x 3 d |
|
| Pregnancy | Amoxicillin
Nitrofurantoin Cephalexin TMP/SMZ Duration: 7 days |
AVOID:
FQ Tetracyclines AG TMP/SMZ (esp 3rd trimester |
Pregnant women should be screened for UTI even if asymptomatic |
| Recurrent cystitis | Relapse: treat 2-6 weeks | Reinfection
<2/yr: pt initiated x3days 3+/yr: post-intercourse TMP/SMZ SS, cephalexin 250mg, nitro 50-100mg 3+/yr: daily or 3x/wk |
3+/yr other can also use TMP 100mg, or Norfloxacin 200mg |
| Uncomplicated Pyelonephritis | Not requiring hospital:
Cipro 500mg BID x 7d Cipro ER 1000mg daily x 7d OR Levo 750 mg daily x 5d OR TMP-SMX DS bid x 14d
Hospitalized: IV FQ Aminoglycoside with or w/o ampicillin OR extended-spectrum cephalosporin or an extended-spectrum pcn with or without an aminoglycoside or carbapenem
|
Not requiring hospital:
Or Oral beta-lactam (less effective) plus initial IV ceftriaxone 1gm OR IV 24-hour dose of aminoglycoside
|
For pts without N/V and not immunocompromised |
| Complicated UTIs | FQ levo x 5 days
AG x 5-14 days |
Extended spectrum Beta lactam | |
| Catheter-related UTIs | Symptomatic pts x 7-10 days and cath removal | Assymptomatic pts should NOT be treated | E.coli, Candida, Enterococcus, Pseudo, Kleb pneumo, Enterobacter |
| Prostatitis | Acute: Duration 4 weeks TMP/SMZ
Cephalosporins FQ |
Chronic: 1-4 months
TMP/SMZ FQ |
|
| Epididymitis | >35 yr: TMP/SMZ, FQ
x 10 days- 4 weeks |
< 35 yr: Ceftriaxone 250mg IM AND doxycycline 100mg bid
x 10 days |
Skin and Soft Tissue Infections
| Cellulitis | Nafcillin, Oxacillin, Dicloxacillin x5-10 days | Alternatives: Clinda, BL combos, 1st ceph | Vanco/Linezolid for MRSA
PCN G if streptococcal |
| Erysipelas | Penicillin G, Clindamycin
x 7-10 days |
||
| Necrotizing Fasciitis | B lactam combo + clinda + cipro
Carbapenems Cefotaxime + clinda OR metron |
Streptococcal: High dose IV PCN + clindamycin | ABX not curative, surgical debridement necessary! |
| DM Foot Infection | Deep: 1-2 weeks
Amp/sulbac, Ticar/clav, Pip/taz Ertapenem FQ + [clindamycin OR metron] Cefoxitin 3rd ceph + [clinda OR metron] |
Shallow: treat like cellulitis
PCN, 1st ceph, etc. |
Topical: Becaplermin 0.01%
Human platelet derived growth factor, improves healing from 35-50%
Surgery also important |
Osteomyelitis: treat for 4-6 weeks (chronic IV 6-8 weeks + 3-12 months PO)
1. Neonates: Nafcillin + [cefotaxime OR AQ]
2. Infants: Cefuroxime OR ceftriaxone OR [Nafcillin + cefotaxime]
3. Peds (>3yr): Nafcillin OR Cefazolin OR Clindamycin
4. Adults: Nafcillin OR Cefazolin OR Vancomycin
5. Pts with Sickle Cell Anemia: Nafcillin + Ampicillin
6. Prosthetic Joint Infections: Vancomycin + rifampin OR Nafcillin + rifampin
CNS Infections: Meningitis
Empiric: 7-14 days
1. Neonates: Ampicillin + AQ OR + cefotaxime
2. 1 month- 50 yrs: 3rd ceph (cefotaxime, ceftriaxone) + Vanco
3. >50 yrs: 3rd ceph +Vanco + ampicillin
4. penetrating head trauma: Vanco + cefepime, ceftazidime, meropenem
Pathogen Known: MOSTLY PCN G 4mill units IV q4h OR Ampicillin 2g q4h, alt: 3rd ceph, vanco, mero, FQ
Corticosteriods: Dexamethasone 0.15 mg.kg q6h x2-4 days; give 10-20 mins before (or at time of ) Abx
Benefit in: Peds with H.flu and Adults with S. pneumo
Brain Abscess: Treat based on source: mostly metron + 3rd Ceph Unknown source: Vanco + Metron+ 3rd ceph
Endocarditis: Strep, Staph, Entero, HACEK Duration: 4-6 weeks (8+ weeks with VRE)
Strep: PCN G ± gent, Ceftriaxone ± gent, Vanco
Staph: Oxa/nafcillin ± gent (+ rifampin if prosthetic valve), Cefazolin ± gent (+ rifampin if prosthetic)
MRSA: Vanco (+ rifampin if prosthetic); may also use Vanco in severe PCN allergy
Entero: [PCN G or ampicillin or vanco] + [gent or streptomycin] VRE: linezolid, Quin/Dalf
HACEK: ceftriaxone, Amp/sulbactam, FQ
PPx: dental and resp tract procedures: Amoxicillin 2g PO 1 hr prior PCN Allergy: Clinda, azith/clarith
Perotonitis/ Intra-Abdominal Infections
Mild-Mod: cefoxitin, Ticar/clav, ertapenem, moxifloxain,tigecycline; [cipro/levo +metronidazole],
[cefazolin/ cefuroxime/ceftriaxone/cefotaxime + metronidazole]
Severe, healthcare acquired, High-risk: Pip/Taz, [ceftazidime/cefepime +metronidazole], imi/cil, mero, dori, [cipo/levo +
metronidazole (not for healthcare acquired)]
Duration: 4-7 days, [injuries repaired in 12hr can be treated for only 24 hr]
C. difficile: diagnose by presence of endotoxins
Initial Therapy: Mild to moderate initial episode: Metronidazole 500mg PO/IV tid x 10-14days OR Vanco 125mg PO QID x 10-14days
Severe initial episode: Vancomycin 125 mg PO QID for 10-14 days
Severe complicated CDI: Vancomycin 500mg PO plus Metronidazole IV 500mg Q8H
Recurrences: First recurrence: Same as for initial episode
Second recurrence: Vancomycin tapered/pulsed
Medical/Surgical PPX
| Procedure | Treatment | Comment |
| Gastric/duodenal | Cefazolin 1-2g | Indicated: morbid obesity, esophe obstruction, decreased gastric pH or motility |
| Biliary | Cefazolin 1-2g | Indicated with (without?): acute cholecystitis, obstr. jaundice, common duct stones, >70yr |
| Appendectomy | Cefoxitin 1-2g
Cefazolin 1-2g + metronidazole OR amp/sulbactam |
If perforated treat x 3-7 days |
| Colorectal | Cefoxitin 1-2g
Cefazolin + metronidazole OR amp/sulbacam Gent/tobra 1.5mg/kg + clinda 600mg/metron 0.5-1g ± neomycin +erythromycin/ metronidazole |
PO/IV may be better bc PO only may cause Cdiff
Mechanical bowel prep is not recommended |
| Obstetrics/GYN | Hysterectomy: Cefazolin/cefoxitin 1-2g
Caesarian: cefazolin 1-2g |
Caesarian: administer AFTER cord clamped |
| Cardiothoracic | Cardiac surg/Pulm resection:
cefazolin/cefur oxime 1-2g Vascular surg: cefazolin 1g q8h x3doses |
For all: Use Vanco if MRSA risk
|
| Orthopedic | Cefazolin 1-2g (or cefur or vanco) | Indicated: surgery involves prosthetics |
| Head/Neck | Cefazolin 1-2g
Amp/sul 1.5-3g Gent 1.5mg/kg + clinda 600-900mg |
Indicated: major surgery when incision through oral or pharyngeal mucosa |
| Urologic | NOT recommended | If (+) urine culture, treat then operate |
 And because pseudomonas is always mentioned:
And because pseudomonas is always mentioned:
| Pseudomonas aeruginosa |
| Drugs of Choice: Piperacillin-tazobactam, Imipenem, Meropenem, Ceftazidime, Cefepime, Amikacin, Gentamycin, Tobramycin, Ciprofloxacin |
| Alternatives: Timentin, Aztreonam, Levofloxacin |
| Third-Line agents: |
| Comments: (Gram-negative bacilli). Consider using two agents from two different classes as empiric treatment in critically ill patients if P. aeruginosa is suspected. Once susceptibilities known, narrow to one drug according to susceptibility report. |